Hard skills include essential technical abilities such as skill in patient monitoring systems, understanding of medical terminology, and competency in emergency procedures.
Package Handler Resume Examples & Templates
Looking to stand out in your job search? Our package handler resume examples will help you showcase essential skills like teamwork, attention to detail, and efficiency to catch employers' eyes.

by Gabriela Hernandez, Last Updated: January 21, 2026
Hired By:*

Popular Package Handler Resume Examples
Discover our top package handler resume examples that emphasize key skills such as efficiency, attention to detail, and teamwork in logistics. These samples demonstrate how to effectively present your qualifications and achievements to potential employers.
Want to build a standout resume? Our Resume Builder offers user-friendly templates specifically designed for those in the logistics industry, making it simple to showcase your strengths.
Recommended
 Customize This Resume
Customize This ResumeEntry-level package handler resume
What this resume does well:
This entry-level resume for a registered nurse position highlights the applicant's clinical skills and relevant experiences gained through rigorous nursing education and practical rotations. New professionals must effectively showcase their competencies in patient care, teamwork, and adaptability to reassure employers of their potential, even with minimal hands-on experience.
Mid-career package handler resume
What this resume does well:
This resume succinctly showcases qualifications that highlight the job seeker’s progression in logistics. The emphasis on efficiency, leadership roles, and safety compliance illustrates readiness for more complex responsibilities within the field.
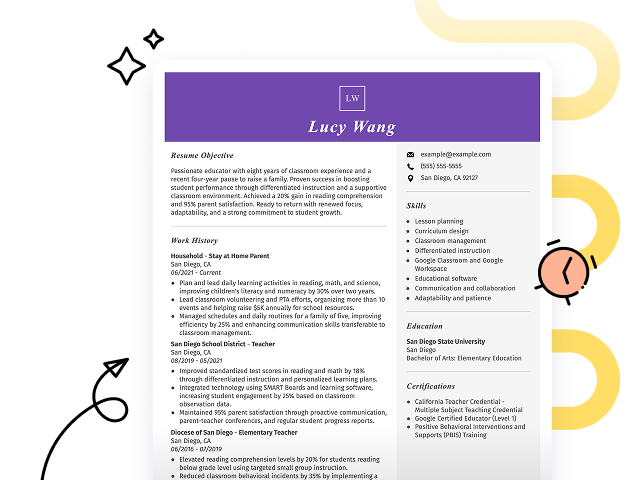
Experienced package handler resume
What this resume does well:
The work history section illustrates the applicant's extensive experience as a package handler, highlighting their management of over 1,500 packages daily with a remarkable 98% accuracy rate. The clear formatting and bullet points improve readability, making it easy for hiring managers to quickly identify key achievements.
Resume Template—Easy to Copy & Paste
Example
John Zhang
Parkview, MO 64158
(555)555-5555
John.Zhang@example.com
Professional Summary
Motivated Package Handler with 4+ years in logistics, skilled in inventory management, shipping coordination, and process optimization, with proven records of efficiency improvement and delivery accuracy enhancement.
Work History
Package Handler
Express Parcels Co. - Parkview, MO
June 2023 - November 2025
- Processed 500+ packages daily efficiently
- Improved loading times by 20%
- Maintained 98% delivery accuracy
Warehouse Associate
LogiTech Industries - St. Louis, MO
January 2022 - May 2023
- Managed inventory worth 200K
- Reduced order errors by 15%
- Streamlined tracking processes
Shipping Clerk
Global Freight Solutions - St. Louis, MO
January 2021 - December 2021
- Coordinated 300+ shipments weekly
- Enhanced shipping procedures
- Ensured timely deliveries consistently
Languages
- Spanish - Beginner (A1)
- French - Intermediate (B1)
- German - Beginner (A1)
Skills
- Inventory Management
- Shipping Coordination
- Time Efficiency
- Delivery Accuracy
- Team Collaboration
- Problem Solving
- Attention to Detail
- Process Optimization
Certifications
- Certified Supply Chain Professional (CSCP) - APICS
- Logistics Management Certification - Institute of Supply Management
Education
Master of Business Administration Operations Management
Illinois State University Normal, Illinois
May 2020
Bachelor of Arts Logistics
University of Illinois Urbana-Champaign, Illinois
May 2018
Build Your Resume in Minutes
Creating a custom resume is easier than ever with our Resume Builder!
How to Write a Package Handler Resume Summary
Your resume summary is the first thing employers will see, making it important to create a powerful introduction that highlights your qualifications. As a package handler, you should emphasize your physical abilities, attention to detail, and experience in fast-paced environments. To help you understand effective strategies, review these package handler resume summary examples that illustrate what works and what doesn't:
Weak Example
I am a dedicated package handler with several years of experience in the industry. I am seeking a position where I can use my skills and contribute positively to the team. A company that values hard work and offers good benefits would be ideal for me. I believe I would make a positive impact if given the chance.
Why this summary misses the mark:
- Contains general statements that do not highlight specific skills or achievements
- Overuses personal pronouns, making it feel less professional and more informal
- Emphasizes what the applicant desires from the job rather than showcasing how they can benefit the employer
Strong Example
Compassionate registered nurse with 7 years of experience in critical care environments, adept at managing high-acuity patients and leading emergency response initiatives. Achieved a 20% increase in patient satisfaction scores by implementing evidence-based practice protocols and fostering effective communication among staff. Proficient in advanced cardiac life support (ACLS), telemetry monitoring, and electronic health record systems.
Why this summary works:
- Begins with specific experience duration and area of expertise
- Highlights a quantifiable achievement that reflects positive patient outcomes
- Mentions relevant technical skills that align with the needs of healthcare employers
Pro Tip
If you’re new to the job market, consider using a career objective rather than a summary. This approach highlights your goals and enthusiasm. Check out various resume objective examples tailored to your field for inspiration and guidance.
Showcasing Your Work Experience
The work experience section is the cornerstone of your resume as a package handler, where you'll focus most of your content. Reputable resume templates will always include this key area.
Your past roles should be listed in reverse-chronological order, with bullet points detailing your accomplishments and duties within each position.
We’ll now look at some examples to help you understand effective and ineffective entries for a package handler's resume. These will highlight what stands out and what misses the mark:
Weak Example
Package Handler
Fast Delivery Services – Atlanta, GA
- Loaded and unloaded packages
- Kept the work area clean and organized
- Followed safety procedures during handling
- Worked with team members to meet targets
Why this work experience section misses the mark:
- No details about the employment dates
- Bullet points are vague and do not showcase specific skills or achievements
- Focuses on basic tasks rather than measurable contributions to team goals
Strong Example
Package Handler
UPS – Atlanta, GA
June 2020 - Current
- Efficiently sort and load an average of 800 packages per shift, ensuring timely dispatch and delivery
- Implement safety protocols that reduced workplace incidents by 30%, improving team compliance and well-being
- Train new hires on operational procedures, contributing to a seamless onboarding process and improving team productivity
Why this work experience section works:
- Each bullet begins with a dynamic action verb that clearly states the job seeker's contributions
- Incorporates quantifiable results to highlight the impact of the job seeker's efforts
- Demonstrates relevant skills such as teamwork, safety awareness, and training abilities
While your resume summary and work experience often take center stage, don’t overlook the importance of other sections. Each part plays a key role in showcasing your qualifications. For more insight into crafting a standout resume, explore our detailed guide on how to write a resume.
Top Skills to Include on Your Resume
A well-defined skills section is important for your resume, as it provides a snapshot of your qualifications to potential employers. This section helps you stand out by showcasing the technical skills that align with the job requirements.
As a package handler, highlight both technical skills and physical abilities. Include experience with pallet jacks, familiarity with warehouse management software, and skill in inventory tracking systems to demonstrate your readiness for fast-paced warehouse operations.
On the other hand, soft skills involve important interpersonal traits like active listening, teamwork, and adaptability that strengthen patient relationships and boost collaboration within healthcare teams.
Selecting the right resume skills is important as it aligns your qualifications with what employers expect from ideal applicants. Many organizations use automated screening tools that filter out applicants lacking essential skills for the position.
To improve your chances of passing these systems, carefully examine job postings to identify which skills are emphasized. This focus not only helps you tailor your resume for recruiters but also ensures it meets ATS requirements effectively.
Pro Tip
To ensure your resume stands out to hiring managers, use our ATS Resume Checker. It identifies over 30 common mistakes, helping you optimize your resume to bypass applicant tracking systems effortlessly.
10 skills that appear on successful package handler resumes
Emphasizing sought-after skills on your resume can significantly boost your chances of catching recruiters' attention. Our resume examples showcase these high-demand abilities, enabling you to apply for jobs with the confidence that a standout resume provides.
By the way, consider adding any relevant skills from the following list that align with your experience and job requirements:
Attention to detail
Problem-solving
Team collaboration
Time management
Adaptability
Customer service orientation
Technical skill
Project management
Data analysis
Creativity
Based on analysis of 5,000+ logistics professional resumes from 2023-2024
Resume Format Examples
Selecting the appropriate resume format is important as it showcases your key skills, relevant experience, and career growth in a clear and compelling way.
Entry-Level 0 - 2 years
Functional
Focuses on skills rather than previous jobs
Best for:
Recent graduates and career changers with up to two years of experience.
Mid-Career 3 - 7 years
Combination
Balances skills and work history equally
Best for:
Mid-career professionals looking to highlight their skills and growth potential.
Experienced 8+ years
Chronological
Emphasizes work history in reverse order

Best for:
Seasoned package handlers with strong expertise in fast-paced logistics environments.
Frequently Asked Questions
Should I include a cover letter with my package handler resume?
Absolutely, including a cover letter can significantly improve your application by showcasing your unique qualifications and enthusiasm for the position. It allows you to personalize your story beyond what's on your resume. If you need assistance crafting yours, explore our detailed guide on how to write a cover letter or use our easy-to-use Cover Letter Generator to help you get started quickly.
Can I use a resume if I’m applying internationally, or do I need a CV?
When applying for jobs abroad, use a CV instead of a resume. A CV provides a comprehensive overview of your academic and professional history, which is often required in international applications. Explore our resources to learn how to write a CV and see CV examples that can help you craft an effective document.
What soft skills are important for package handlers?
Soft skills like communication, problem-solving, and collaboration are essential for package handlers. These interpersonal skills foster teamwork and ensure efficient operations, enabling handlers to work effectively together and maintain smooth logistics processes.
I’m transitioning from another field. How should I highlight my experience?
Highlight your transferable skills, such as communication, teamwork, and adaptability, to showcase your value in Package Handler roles. Even if you lack direct experience, these abilities can significantly improve your suitability. Provide concrete examples from previous jobs that align with the responsibilities of the position to demonstrate how you can make a positive impact.
Should I use a cover letter template?
Yes, using a cover letter template tailored for registered nurses improves your ability to present your clinical skills and patient care experience clearly. This approach ensures organized content that emphasizes key achievements like certifications or successful patient outcomes, which catch hiring managers' attention.
Should I include a personal mission statement on my package handler resume?
Including a personal mission statement on your resume can effectively convey your values and career aspirations. This approach is especially useful when applying to organizations with strong cultural or mission-driven focuses, as it highlights alignment with their core principles.

Ready to land the job?
Join 28M+ others who've built a resume that works.